There is another way: Clinical simulation
 Dr Teresa O'BrienFollow 7 min read · December 9, 2025
Dr Teresa O'BrienFollow 7 min read · December 9, 2025
In this microlearning, you will:
- Identify the purpose and core methods of clinical simulation research in digital health.
- Analyse a healthcare case study to map how a simulation study is set up, run, and evaluated.
- Evaluate the benefits of simulation studies for digital-health interventions.
This microlearning is a part of a set of learnings in our Project Incubator. If you enjoy this learning, please explore The Validitron page to see how you can develop your digital health project with us and the Learn page to see our other education offerings.
What comes to mind when
you hear the word “Simulation”?
When you think of simulation, many things may come to mind. Pop culture has explored the concept in films such as The Matrix and The Truman Show. The gaming industry has created a simulator for almost any experience you can imagine. "Goat Simulator" has over 50 million downloads on the Google Play Store!
Beyond entertainment, simulations are often seen as computational tools to model complex systems like traffic or climate, and in clinical settings as role-play for teaching.
While simulations span entertainment, computation, and training, this micro-learning examines simulation as an evidence-generation method for digital health. A use you may have never considered.
Simulation is a technique to replace or amplify real experiences with guided experiences that evoke or replicate the real world interactively. — Gaba, 2004
New technologies, old methodologies
Today, randomised controlled trials (RCTs) are the gold standard for determining whether a new drug works and for whom. This method was established in the 1940s, when advances in chemistry began bringing a range of new ‘miracle’ pharmaceuticals to medicine, including antibiotics, to treat diseases. Scientists needed the right method to understand what works, and established the drug development process we know today.
In 2025, we are well and truly in the digital transformation of health, with new digital technologies being developed every day. Mirroring the 1940s, researchers worldwide are now realising that we need new, fit-for-purpose methods to generate the right evidence at the right time to determine whether a digital technology is safe, effective, useful, and appropriate for healthcare.
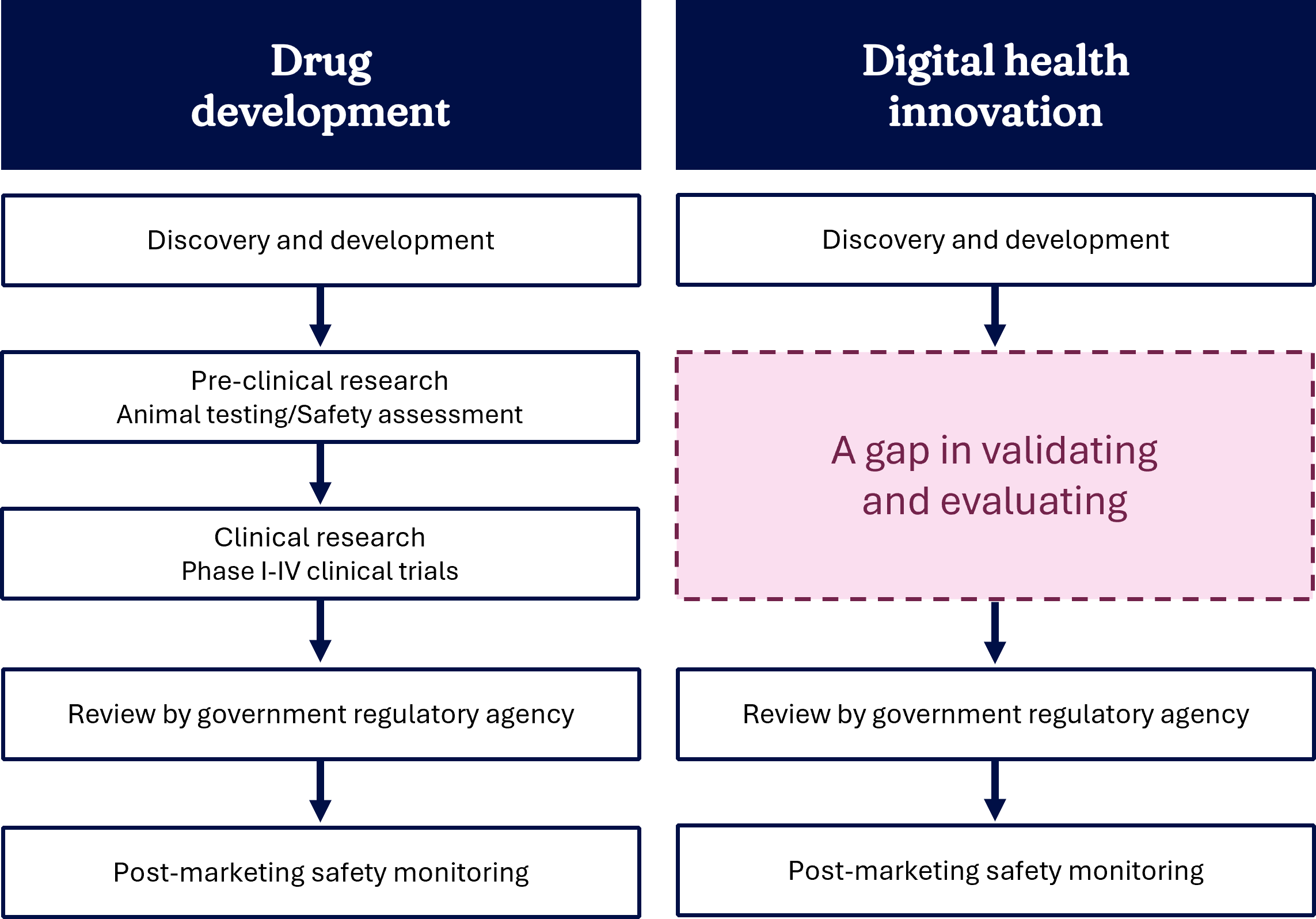
Most of us know that to create a digital health tool, we need to use co-design with end users and implement it into the real world. Clinical simulation is the essential evidence generation method that sits between these two stages.
We have a lot of examples of when these digital health tools don’t work for various reasons. For example, poor workflow fit is a key determinant of non-use attrition and consequent adoption failure in clinical decision support systems, but is rarely identified before implementation. Poor workflow fit makes healthcare staff 50% less likely to use decision support systems (Rosenberg et al., 2022).
There is more and more evidence that design and workflow fit validation activities should be undertaken early in the development to allow timely changes, which is where simulation comes in.
Most consumers abandon digital health apps after only 5.5 days because they find them too burdensome. — Pratap et al., 2020
How does simulation work?
Have you ever played with a kitchen set as a child? You picked up a toy pan, pretended to cook pancakes, and served them to your family and friends. It wasn’t real, but it felt real enough to explore it as if it were real—without the heat of a real stove or electric components. That’s what simulation does: it creates a safe, controlled environment where you can explore, test, and practice without real-world consequences. It’s not reality, but it prepares you for it.
In our context, clinical simulation refers to simulation:
- Performed by real users, e.g., clinicians
- Enacting realistic clinical work scenarios, e.g., consultation with a patient
- In close to real-life environments, e.g., in a clinical consultation room or a hospital ward.
(Jensen, 2014)
We use established frameworks, such as the Input–Process–Output (IPO) framework, to guide the design of a simulation:
- Input involves defining the problem and confirming whether clinical simulation is the right approach.
- Process focuses on designing and delivering the simulation, and collecting and analysing data.
- Output covers reporting findings, identifying key recommendations, and reviewing the impact of the simulation for future projects.
Practically, let's follow how we would conduct a simulation. Flip each card for more information:
But what's your question?
You've seen that defining a good research question is an important planning step for a clinical simulation. You're probably wondering what kinds of questions are possible. In fact, simulation offers flexibility to answer a wide range of questions focused on de-risking digital health:
- Design: Role-playing through a typical work situation, where might a digital health tool be needed? What works well that shouldn't be changed?
- Usability: Can users successfully complete tasks, find information, and navigate through a prototype of a digital health tool as part of their normal work?
- Acceptability: Having experienced a digital health tool in action, what wider opportunities or challenges do users see around it being introduced?
- Patient-centredness: How does the introduction of a new digital health tool affect patient-clinician communication and experience within a typical consultation?
- Safety: What proportion of users can use a decision support tool correctly in a realistic work situation? Observing users at work with a digital health tool, are there new or latent safety issues that need to be addressed?
- Efficiency: How long does it take users to complete tasks using a digital health tool in a realistic, but controlled, environment?
Common to all of these is the ability to test technology in a controlled but realistic setting without putting patients at risk.
 Incubator activity
Incubator activity
Think about:
- A digital health tool you have used that didn’t quite work. What caused the frustration—poor fit with your workflow, unclear interface, wrong timing, or something else? What similar risks might affect your own project?
- A realistic clinical scenario in which your digital health tool would be used. Who is involved? What steps occur before, during, and after? Identify at least one workflow point where things could go wrong.
Simulation in action
Let's follow the process of simulation using a real example. Select the next arrow to move through each stage of the scenario.
After the simulation, we had an optimised tool ready for real-world evaluation. We ensured the real-world evaluation measured the right outcomes, and we had valuable pre-implementation information. This tool is now being rolled out around Australia for telehealth.
Clinical simulation can help gather evidence quickly and allow for changes to the tool, leading to an improved final product that is more likely to be adopted and effective. It is more cost-effective to fail early rather than to implement and then fail.
It is also increasingly recognised by regulatory bodies like the FDA for making market authorisation decisions for software as a medical device.
Exploring the simulation space
Let’s take a tour of the Validitron simulation space. When you’re ready, select "Start the tour". In each room, look for the 👁️ icons, select them to learn more.
Key takeaways
Clinical simulation:
- Is an immersive, inexpensive, and rigorous method for evaluating emerging digital health innovations in a low-risk environment, before real-world testing.
- Enables researchers to test innovations within realistic clinical environments to explore issues such as workflow fit, human factors, and trust.
- Allows various clinical scenarios involving diverse patient and clinician personas to be simulated to understand better user preferences, potential usability challenges, workflow-related acceptance and implementation issues, and other human factor considerations.
- Supports psychological safety for participants.
References:
- Gaba, D. M. (2004). The future vision of simulation in health care. Quality & Safety in Health Care, 13(Suppl 1), i2–i10. https://doi.org/10.1136/qhc.13.suppl_1.i2
- Pratap, A., Neto, E. C., Snyder, P., Stepnowsky, C., Elhadad, N., Grant, D., Mohebbi, M. H., Mooney, S., Suver, C., Wilbanks, J., Mangravite, L., Heagerty, P. J., Areán, P., & Omberg, L. (2020). Indicators of retention in remote digital health studies: A cross-study evaluation of 100,000 participants. NPJ Digital Medicine, 3, 21. https://doi.org/10.1038/s41746-020-0224-8
- Rosenberg, J., Miller, K., Pickard, O., Henrich, N., Karlage, A., & Weintraub, R. (2022). Barriers and facilitators to use of a digital clinical decision support tool: A cohort study combining clickstream and survey data. BMJ Open, 12(11), e064952. https://doi.org/10.1136/bmjopen-2022-064952